Justin Myers | January 26, 2021
View PDF
Introduction
"Why can't the greatest economy in the history of the world produce swabs, face masks, and ventilators in adequate supply?" asked Dr. Laurence Summers, former director of the National Economic Council and Chief Economist at the World Bank, in March 2020.1 This concern was shared throughout the United States: did globalization cripple the greatest economy in the world? The COVID-19 pandemic was a systemic shock that broke global supply chains.2 The United States was and continues to be unable to provide enough essential protective equipment to healthcare providers, leading to calls for targeted policies to re-shore medical manufacturing in the interest of national security.3 These proposals, while attempting to address a real issue with the shortcomings of medical supply chains in other countries, are unlikely to address the underlying causes of the personal protective equipment (PPE) shortages in the United States during the pandemic.
Background
Medical supply chains have followed the path of much of the rest of the American manufacturing industry. Kimberly-Clark and Honeywell, two of the United States’ largest medical manufacturers, moved much of their PPE manufacturing to China in the early 2000s.4 Personal protective equipment is similar to mass-produced apparel or common commodities; it is a low margin good that can be mass produced at a low cost using little intellectual property. These attributes made it a good candidate for offshoring to cheap labor markets. Cheap labor, easy access to raw materials, and the opportunity to enter the new Chinese medical market as the country’s massive population opened to western markets motivated firms to move to the growing country. Medicine manufacturing was also moved overseas: ninety percent of the United States’ antibiotics and 75% of its acetaminophen is sourced abroad. Opaque record keeping makes exact numbers hard to pin down, but studies have also indicated 80%5 of the raw materials for all U.S. drugs are sourced from China.6 Forty-eight percent of the United States’ PPE in 2019 was manufactured in China, including 95% of surgical procedure masks, 97% of plastic gloves, and 70% of its N95 respirators, per the Department of Health and Human Services.7 Major medical supply companies still have significant manufacturing capacity in the United States (3M has several large manufacturing plants in the Midwest), but these plants could not fulfill much of the U.S. demand for PPE under normal circumstances.8 Moving these supply chains abroad was driven by reducing costs, as was the introduction of the “just-in-time” (JIT) inventory management strategy.9 JIT lowered prices but meant most health systems purchased just enough PPE for what they needed10, plus an extra 15-30 days of supplies.11 However, this meant the goods traveled on a fragile supply network originating half a world away to make it to U.S. hospitals mere days before they were needed.12 Breakdowns at any point in the chain would put pressure on healthcare providers13, but that pressure was usually alleviated by buying temporarily from a different supplier in a different region.
Congress established the Strategic National Stockpile (SNS) in 1999 to hedge against surges in demand for pharmaceutical products (for more information on the SNS, see Appendix B).14 Originally intended to be a stockpile for vaccines, it was expanded to all emergency equipment in 2000. The SNS is composed of a network of warehouses across the United States, each stocked with various necessary emergency and medical supplies in case of a biological or chemical attack or a natural disaster. Congress originally allotted $51 million to start the SNS, but the agency’s annual funding plateaued in the late 2000s near $700 million.15 That money paid for the upkeep and acquisition of new materials for the SNS, but the focus of the organization was on preparing for a single mass casualty event, not a prolonged health crisis.16 An independent study of American pandemic readiness in 2016 indicated that healthcare providers thought they could rely on the SNS to help with surge capacity of PPE in a pandemic situation.17 This was not true: the goal of the SNS was to be a short-term, temporary stopgap for a one-time event and the actions and acquisitions of the agency were not aimed at any broader support.18
The emergence of H5N1 in 1997, SARS in 2003, the Swine Flu in 2009, MERS in 2012, and an Ebola outbreak in 2015 incentivized the Federal government to invest in pandemic ‘insurance’ (contingency plans and funding for the SNS) for the past 20 years.19 The first multi-agency “Pandemic Preparedness Report” was issued in 2005. Since then, the job of preparing for an outbreak was the bureaucratic backwater of the Department of Homeland Security (and then the DHHS).20 These reports considered some of the necessary logistics involved in coordinating a pandemic response, but overlooked the details of retooling U.S. medical supply chains or stockpiles. Some reports discussed the federal responsibility to coordinate the equipment distribution, but none laid out what that process might look like. The authority for such preparations shuffled between different agencies, even as the SNS continued to respond to small viral epidemics. The SNS stocked up on U.S. goods slowly over time, and (reportedly) had almost 90 million N95 respirators on hand in 2009.21 However, they distributed most of that inventory during the H1N1 epidemic in 2009/10, and had fewer than 25 million respirators (some estimates were as low as 12 million) and 20,000 ventilators in stock entering 2020.22 Independent23 and government experts estimated in 2017 and 2018 that the United States would need upwards of 3 billion N95 respirators for a year-long pandemic, using conservative estimates of illness and PPE reuse.24
When the first warnings about COVID-19 emerged in January 2020, domestic PPE producers launched into action, boosting capacity and trying to import as much PPE as possible.25 But the United States didn’t initially have enough surge capacity for all of the necessary goods, and still relied on imports to bolster its PPE stock.26 By February, Chinese manufacturers were ordered by the Chinese Communist Party to halt all PPE exports27 and to focus on the domestic market.28 The U.S. healthcare system began to face a shortage of key equipment,29 even before the initial wave of COVID-19 washed over the United States in late March (the 15-30-day supply of PPE began to run out in some healthcare systems before some hospitals saw their first case).30
The Trump administration entered office in 2016 promising to remake the world order in a way that favored the United States. It placed tariffs on foreign countries, particularly China, in 2018 (and eventually 2019), claiming national security required the protection of certain key industries and trying to punish China for unfair trade practices.31 USTR Robert Lighthizer argued the United States needed to protect and maintain key domestic manufacturing supply chains in case of war or disaster.32 The tariffs the administration placed on Chinese (and some other foreign) goods covered a broad swath of products, including several key pieces of PPE, drugs, and ventilators.33 In spite of opposition from the medical supply industry, which argued it would simply raise prices instead of providing protection or reshoring, the tariffs were implemented.34 The Peterson Institute’s Dr. Chad Bown estimates those tariffs caused movement in medical supply chains, but not back into the United States.35 Instead, manufacturers sought cheap labor elsewhere in Asia. These tariffs, ranging from 15% to 25%, significantly impeded the U.S. healthcare systems’ ability to cheaply procure PPE in the 18 months leading up to and during the COVID pandemic.36 Many hospitals dug into their stockpiles in 2018 and 2019 to help cover the extra cost of the tariffs on the goods, leaving their already scant stockpiles depleted entering 2020.37
Analysis
The United States can’t allow a supply chain crisis like that of spring 2020 to occur again. Most nations across the world initially struggled to find PPE, instituting temporary protectionist measures to make sure their domestic supply of PPE was available to their healthcare industries. But in the United States, the shortage of PPE has been chronic and consistent since February 2020.38 One solution presented by various policy analysts, commentators, and politicians has been to introduce reshoring policies to draw key manufacturing back to the United States.39 Some of these policies are narrow and targeted; subsidies for certain counties in New York, for instance.40 Others are broad, resembling President Trump’s trade war strategy of recent years with tariffs, quotas, and other non-tariff barriers being used to drive profit margins down for companies until they are forced to return to the United States.41
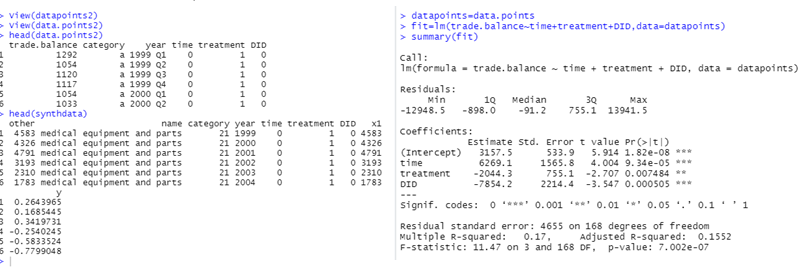
Broadly speaking, the 2018-19 tariffs caused an acceleration of the reshoring and nearshoring manufacturing trend that was already growing as wages and costs rose in China.42 However, much of this reshoring was driven by high tech manufacturing returning home; commoditized goods, such as masks, gowns, and generic drugs were still able to be cheaply produced in China and did not reshore in response to the Trump administration’s policies.43 A graphical analysis comparing the trends of the medical supply industry trade balance to other industries that were hit by tariffs can be seen in Figure 1. The blue Kearney Reshoring Index saw a sharp spike after the policies were implemented, indicating an increase in businesses moving home, but the medical supply industry and the engine parts industries (both largely commoditized) continued their negative trend.44 Statistical analysis using control groups (both real and synthesized with the statistical program R) illustrate further that the Trump administration’s did nothing to stop the previously-established trend of increased trade deficits in the medical supply industry.
Figure 1
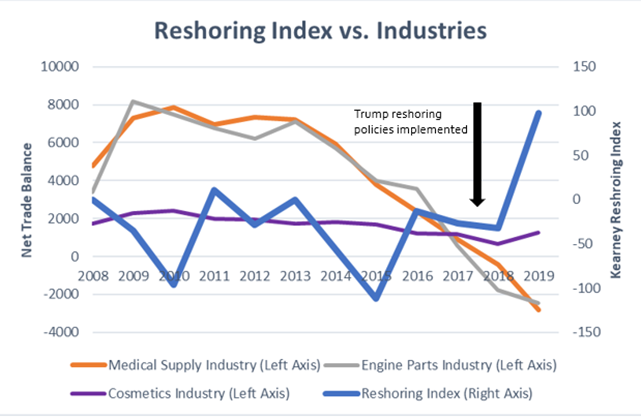
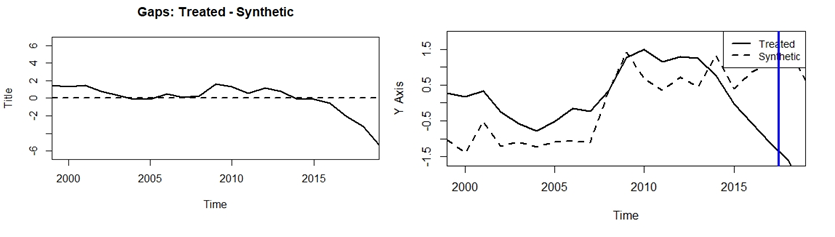
Figure 2
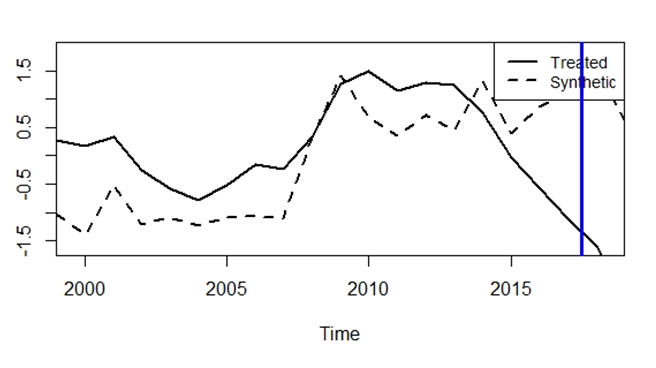
R synthesized control industry compared to medical supplies industry
illustrates no reversal in trade balance trend
The synthetic industry and the real control industries, which had similar trends before the tariffs, continued their divergence in a statistically significant way after the tariffs were implemented. The United States will be unable to bluntly “tariff” its way into reshoring the medical supply industry due to the nature of the commoditized goods it is trying to bring home. A more complex system of subsidies for domestic manufacturers would be required to accomplish that goal, which would have to be sustained over time, even if there is not another similar global health crisis for decades.
Reshoring capacity may be possible with the right subsidies program, but it may not be sustainable without significant and unnecessary inefficiencies.45 During the H1N1 epidemic in 2009, the nation’s remaining PPE manufacturers saw an increase in demand for their goods; many invested in further domestic capacity, anticipating demand for their goods being needed again.46 However, this glut of supply overran the U.S. market, and caused healthcare systems to stockpile the cheap equipment in 2010, depressing demand in the following year and causing significant harm to domestic manufacturers.47 This inability to flex surge capacity in the U.S.’ domestic production indicates the key problem with reshoring: the capacity needed to fulfill demand created by a respiratory pandemic can’t be sustained after the initial demand wears off.48 Under normal circumstances, the United States has enough domestic production capability to flex its capacity slightly in response to small outbreaks, but not to a major epidemic or pandemic outbreak. 3M’s management went out of its way to add inefficient surge capacity in case of a major health event following the SARS outbreak, but it was still not nearly enough to make up for the immense demand for PPE that spiked within weeks of the first clusters of COVID-19 cases.49 It is also still generally cheaper to manufacture PPE goods abroad, due to their commoditized nature. The United States can either pay for an expensive program to attempt to subsidize even more of this moth-balled domestic production in the face of low foreign costs, or it can increase its stockpiling and logistical capacity, using the manufacturing capacity already in the United States.50
Outlook
The collapse of the U.S. medical supply chain in the face of the deadliest pandemic in a century was not caused by any singular policy or decision. Rather, the combination of offshoring supply chains into an authoritarian host country, the use of “just-in-time” inventory systems that left no slack in U.S. PPE stocks, healthcare systems’ poor understanding of the United States’ SNS, the lack of funds provided for the SNS to replenish its PPE stocks after the H1N1 epidemic, and the absence of any coordination between the Federal government (and specifically FEMA/SNS) and state health systems to distribute the rare PPE equipment caused the disastrous shortage of PPE and medical equipment in the United States during the COVID pandemic. Preventing such a crisis in the future will require more than a single policy, but the federal government should focus on finding ways to guarantee demand for the industry in the event of a crisis and building stockpiles of goods far larger than those in the pre-COVD world.
Reshoring is not a viable long-term solution to the shortfalls of the medial supply network. The United States can’t use blunt trade instruments like tariffs to bring back key manufacturing lines, and using specific, subsidy-based programs to reshore specific suppliers would create excess domestic capacity that would go unused until the next crisis. A more efficient way of preparing for a demand surge for medical supplies in the future would be to eliminate uncertainty for businesses in the medical supply chain, stockpile the necessary equipment in both regional and local warehouses, and create a distribution network that connects buyers and sellers in a way that prioritizes the areas with the most need in the future. Specific recommendations include:
- The U.S. federal government should increase funding for its medical stockpiles by billions of dollars after the COVID-19 pandemic, funding both the centralized SNS and hospital-level emergency stockpiles. These acquisitions should be purchased from U.S.-based manufacturers to support existing domestic suppliers’ post-pandemic demand surge. Stockpiling allows the U.S. to hedge against unlikely events and support the post-crisis industry without using overly distortionary measures in the global economy. Guaranteeing consistent demand is the end goal.
- The DHHS should create (or, using the small network put in place in late summer 2020, significantly improve51) the organizational network necessary to coordinate the distribution of medical supplies in the event of another prolonged public health crisis. This network would be for emergency use only and would allow local health departments to submit information and needs on one side of a platform. The Federal government would then require reputable medical manufacturers and suppliers to sell their goods only through the platform (using Defense Protection Act authority) to the highest-priority health systems and states. The federal government is the only actor with the authority and the ability to coordinate the national distribution of goods to these hotspots, something it failed to do during the COVID-19 pandemic. This marketplace should guarantee government demand during a crisis, eliminating uncertainty for businesses unsure there are customers for their goods.
- The U.S. government should create a list of key medical items and supplies it considers “essential” and make them ineligible for future trade barriers in an effort to provide some degree of stability to the supply chain and avoid the disastrous effects to U.S. stockpiles pre-COVID.
- Some reshoring will happen organically as the result of accelerating trends in the past and U.S. suppliers’ concerns about losing access to certain supply chains that are heavily concentrated in one country or geographic area. The U.S. should not discourage this movement, but should focus on emphasizing its commitment to stable medical supply chains. In the past, the SNS has done this with specific expensive niche drugs (such as the therapy for botulism): guarantee demand to ensure suppliers will always be ready to surge production if needed. Supporting the industry without explicitly paying subsidies allows for creative destruction but also helps mitigate the risk of the entire market ceasing to exist.
Appendix A: Methodology
To study the efficacy of the reshoring policies on medical supply chains and their possible use in the future to push for reshoring, I used time-series data on U.S. imports, exports, and trade balances from the Bureau of Economic Analysis52 and the United States International Trade Commission.53 For data on the medical manufacturing market in the United States, I used IBIS World data.54 To measure the reshoring policies' impact, I used the Kearney Group's reshoring index based on the manufacturing import ratio (MIR).55 The MIR aggregates imported manufactured goods from 14 Asian trading partners with cheaper labor divided by U.S. domestic output of manufactured goods. I used individual NTS product codes and aggregated product lines to compare reshoring trends to specific PPE goods' trade trends in recent years. I also used both difference-in-differences linear regression analysis and the R package "Synth" to compare the industry to control groups, both real and synthetic, before and after the implementation of the reshoring policies.56
Appendix B: The Strategic National Stockpile’s Response
Congress established the Strategic National Stockpile (SNS) in 1999 to hedge against surges in demand for pharmaceutical products.57 Originally intended to be a stockpile for vaccines, it was expanded to all emergency equipment in 2000. The SNS is composed of a network of warehouses across the United States, each stocked with various necessary emergency and medical supplies in case of a biological or chemical attack or natural disaster. Congress originally allotted $51 million to start the SNS, but the agency’s funding plateaued in the late 2000s near $700 million.58 The money was used for the upkeep and continued acquisition of materials for the SNS, but the focus of the organization went towards preparing for a single mass casualty event, not a prolonged health crisis.59 The SNS had shipping containers full of medical goods sitting, ready to send to crisis areas, but not over a long period of time.60 The SNS stocked up on U.S. goods slowly over time, and (reportedly) had almost 90 million N95 respirators on hand in 2009, right before the H1N1 outbreak.61 However, they distributed most of that inventory in 2009, and had fewer than 25 million respirators (some estimates were as low as 12 million) and 20,000 ventilators in stock entering 2020.62 Independent63 and government experts estimated in 2017 and 2018 that the United States would need upwards of 3 billion N95 respirators for a year-long pandemic, using conservative estimates of illness and PPE reuse; the SNS and U.S. supply chain fell far short of that figure.64 Former administrators65 and experts blamed this shortfall on a lack of money and a focus on purchasing rare, quickly expiring antiviral drugs instead of replenishing the stock of PPE.66 An independent study of American pandemic readiness in 2016 indicated to administrators that healthcare providers thought they could rely on the SNS to help with surge capacity of PPE in a pandemic situation.67 This was not true: the goal of the SNS was to be a short-term, temporary stopgap for a one-time event and the actions and acquisitions of the agency were not aimed at any broader support.68
FEMA initially used the SNS to ship PPE and experimental antivirals to COVID hotspots in early 2020.69 But with a diminished stockpile of PPE and medical supply chains dead in the water, healthcare systems were left with few options when those supplies ran out.70 The Federal government, lacking preparation for the logistics debacle it faced, handed the responsibility for PPE, testing, and ventilator acquisitions to state governments.71 This meant states, major hospital systems, and the SNS began bidding against one another in the market for key medical supplies, driving prices up by a factor of 10 and leading to immense public frustration and danger for healthcare workers who found themselves without the appropriate protection from a deadly respiratory disease.72 The already limited supply was price gouged because of artificial market demand created by government entities bidding against one another. The stories of hospital administrators traveling across the country in unmarked trucks to meet ‘gray market’ dealers with shipments of PPE, trying to avoid FEMA seizure for ‘redistribution’, read more like a third world country’s experiences than those of the most powerful economy in the world.73 While the summer months saw better cooperation between health systems and states, massive shortages of PPE supplies still plague the U.S. healthcare system entering the winter months as case counts edge ever higher.74
_________________________________
Endnotes
Laurence Summers, Twitter, March 21, 2020, https://twitter.com/lhsummers/status/1241329121768230912?lang=en
Muhammad Suhail Rizwan, Ghufran Ahmad, Dawood Ashraf, “Systemic risk: The impact of COVID-19,” Finance research letters vol. 36 (2020): 101682. doi:10.1016/j.frl.2020.101682
David Adler and Dan Breznitz, “Reshoring Supply Chains: A Practical Policy Agenda,” American Affairs, Summer 2020, https://americanaffairsjournal.org/2020/05/reshoring-supply-chains-a-pr…
Yuki Noguchi, “Not Enough Face Masks Are Made In America To Deal With Coronavirus,” NPR, March 3, 2020, https://www.npr.org/sections/health-shots/2020/03/05/811387424/face-mas…
Anna Eshoo and Adam Schiff, “China’s grip on pharmaceutical drugs is a national security issue,” The Washington Post, September 10, 2019, https://www.washingtonpost.com/opinions/we-rely-on-china-for-pharmaceut…
Danielle Pletka and Derek Scissors, “We’re too dependent on China for too many critical goods, especially medicine,” The Dispatch, March 5, 2020, https://thedispatch.com/p/were-too-dependent-on-china-for-too
Tom Simonite, “How Decades of Offshoring Led to a Mask Shortage in a Pandemic,” WIRED, March 29, 2020, https://www.wired.com/story/decades-offshoring-led-mask-shortage-pandem…
Brian Gruley and Rick Clough, “How 3M Plans to Make More Than a Billion Masks By End of Year,” Bloomberg Business, March 25, 2020, https://www.bloomberg.com/news/features/2020-03-25/3m-doubled-productio…
Lizzie O’Leary, “The Modern Supply Chain Is Snapping,” The Atlantic, March 19, 2020, https://www.theatlantic.com/ideas/archive/2020/03/supply-chains-and-cor…
Olga Khazan, “Why We’re Running Out of Masks in the Coronavirus Crisis,” The Atlantic, April 10,2020, https://www.theatlantic.com/health/archive/2020/04/why-were-running-out…
David Freeman, “How 3M Blew Its Reputation on the N95 Mask,” Medium, August 19, 2020, https://marker.medium.com/how-3m-gambled-its-reputation-on-the-n95-mask…
Bolter and Robey, “Strategic Reshoring”, July 1, 2020
Bernard Wysocki Jr. and Sarah Lueck, “Just-in-Time Inventories Make U.S. Vulnerable in a Pandemic,” The Wall Street Journal, January 12, 2006, https://www.wsj.com/articles/SB113703203939544469
Greg Burel, “The Early Years: Shaping a National Stockpile for Preparedness,” Domestic Preparedness, October 9, 2019, https://www.domesticpreparedness.com/healthcare/the-early-years-shaping…
Greg Burel, “Evolving the Scope of the Strategic National Stockpile,” Disaster Preparedness, November 27, 2019, https://www.domesticpreparedness.com/healthcare/evolving-the-scope-of-t…
Greg Burel, “Looking Ahead: The Future of the Strategic National Stockpile,” Disaster Preparedness, December 25, 2019, https://www.domesticpreparedness.com/healthcare/looking-ahead-future-of…
Joshua Hersh, “US Classified Stockpile”, March 17, 2020 Hersh, J., “The U.S. Has a Classified Stockpile of Ventilators and Masks, But It Won’t Save Us From Coronavirus”, Vice News, March 17, 2020, https://www.vice.com/en/article/n7j5bq/the-us-has-a-classified-stockpil…
Nell Greenfieldboyce, “Inside A Secret Government Warehouse Prepped For Health Catastrophes,” NPR, June 27, 2016, https://www.npr.org/sections/health-shots/2016/06/27/483069862/inside-a…
Simonite, T., “Decades,” March 29, 2020
Homeland Security Council, “National Strategy for Pandemic Influenza,” November 2005, Department of Homeland Security, https://www.cdc.gov/pandemic-flu/media/pandemic-influenza-strategy-2005…
Doug Bock Clark, “Inside the Chaotic, Cutthroat Gray Market for N95 Masks,” New York Times, November 17, 2020, https://www.nytimes.com/2020/11/17/magazine/n95-masks-market-covid.html
Hersh, J. “US Classified Stockpile,” March 17, 2020 Hersh
Anita Patel, Maryann M. D'Alessandro, Karen J. Ireland, W. Greg Burel, Elaine B. Wencil, and Sonja A. Rasmussen. “Personal Protective Equipment Supply Chain: Lessons Learned from Recent Public Health Emergency Responses,” Health Security, Volume: 15 Issue 3, Jun 2017.244-252.http://doi.org/10.1089/hs.2016.0129
Cristina Carias, Gabriel Rainisch, Manjunath Shankar, Bishwa B. Adhikari, David L. Swerdlow, William A. Bower, Satish K. Pillai, Martin I. Meltzer, Lisa M. Koonin, “Potential Demand for Respirators and Surgical Masks During a Hypothetical Influenza Pandemic in the United States,” Clinical Infectious Diseases, Volume 60, Issue suppl_1, May 2015, Pages S42–S51, https://doi.org/10.1093/cid/civ141
Gruley, B., and Clough, R., “How 3M Plans,” March 25, 2020
Freeman, D., “How 3M Blew Its Reputation,” August 19, 2020
Martha Mendoza and Juliet Linderman, “Imports of medical supplies plummet as demand in U.S. soars,” AP Wire, March 20, 2020, https://apnews.com/article/6d9382c1e8ee36f9ed1a4dfe7815ceb1
Kate O’Keeffe, Liza Lin and Eva Xiao, “China’s Export Restrictions Strand Medical Goods U.S. Needs to Fight Coronavirus, State Department Says,” The Wall Street Journal, April 16, 2020, https://www.wsj.com/articles/chinas-export-restrictions-strand-medical-…
House Committee on Oversight and Reform, “New Document Shows Inadequate Distribution of Personal Protective Equipment and Critical Medical Supplies to States,” U.S. House Oversight, April 8, 2020, https://oversightdemocrats.house.gov/news/press-releases/new-document-s…
Maryn McKenna, “Amid Coronavirus Fears, a Mask Shortage Could Spread Globally,” Wired, February 4, 2020, https://www.wired.com/story/amid-coronavirus-fears-a-mask-shortage-coul…
Simon Lester and Huan Zhu, “Closing Pandora’s Box: The Growing Abuse of the National Security Rationale for Restricting Trade,” CATO Institute, June 25, 2019, https://www.cato.org/publications/policy-analysis/closing-pandoras-box-…
Robert Lighthizer, “Statement by Ambassador Robert E. Lighthizer on Retaliatory Duties,” USTR.gov, June 26, 2018, https://ustr.gov/about-us/policy-offices/press-office/press-releases/20…
Chad Bown, “Trump's trade policy is hampering the U.S. fight against COVID-19,” The Peterson Institute of International Economics, March 13, 2020, https://www.piie.com/blogs/trade-and-investment-policy-watch/trumps-tra…
USTR 301 Committee, “Section 301 Tariffs Public Hearing,” USTR.gov, August 20, 2018, https://ustr.gov/about-us/policy-offices/press-office/press-releases/20…
Bown, “Trump’s trade policy,” March 13, 2020
Barry Hochfelder, “In US-China tariff poker game, health supply chains stand to lose,” Supply Chain Dive, May 15, 2019, https://www.supplychaindive.com/news/us-china-tariff-health-supply-chai…
Deborah Abrams Kaplan, “How tariffs ravaged the COVID-19 medical supply chain,” Supply Chain Dive, May 27, 2020, https://www.supplychaindive.com/news/coronavirus-tariffs-trade-medical-…
Monika Evstatieva, M., “A Revamped Strategic National Stockpile Still Can't Match The Pandemic's Latest Surge,” NPR, November 23, 2020, https://www.npr.org/2020/11/23/937978556/a-revamped-strategic-national-…
David Adler and Dan Breznitz, “Reshoring Supply Chains: A Practical Policy Agenda,” American Affairs, Summer 2020, https://americanaffairsjournal.org/2020/05/reshoring-supply-chains-a-pr…
Andrew Fish and Honora Spillane, “Reshoring advanced manufacturing supply chains to generate good jobs,” Brookings Institute, July 23, 2020, https://www.brookings.edu/research/reshoring-advanced-manufacturing-sup…
Doug Palmer and Ryan Heath, “How Trump is using coronavirus to reshape world trade,” Politico, May 15, 2020, https://www.politico.com/news/2020/05/15/trump-coronavirus-world-trade-…
Ana Swanson and Jim Tankersley, “The Pandemic Isn’t Bringing Back Factory Jobs, at Least Not Yet,” New York Times, July 22, 2020, https://www.nytimes.com/2020/07/22/business/economy/coronavirus-globali…
Bown, “Trump’s trade policy,” March 13, 2020
Vida Vanchan, Rachel Mulhall, and John Bryson, “Repatriation or Reshoring of Manufacturing to the U.S. and UK,” Growth and Change, Volume 49, Issue 1, March 2018, Pages 97-121. https://doi.org/10.1111/grow.12224
Caroline Freund, “Governments Could Bring Supply Chains Home. It Would Defy Economic Rationality.” Barron’s, May 1 2020, https://www.barrons.com/articles/will-supply-chains-come-home-after-the…
Joel Rose, “NPR Probes Why Personal Protective Equipment Is Still In Short Supply”, NPR, September 16, 2020, https://www.npr.org/2020/09/16/913448230/npr-investigates-why-the-short…
McKenna, M., “Amid Coronavirus Fears,” February 4, 2020,
Susan DeVore, “Surviving The Waves Of A Pandemic Storm: How To Fix The Supply Chain Flaws Exposed By COVID-19,” Health Affairs, September 30, 2020, DOI: 10.1377/hblog20200928.305253
Freeman, D., “How 3M Blew Its Reputation,” August 19, 2020
Rick Dana Barlow, “What. Went. Wrong?” Healthcare Purchasing News, July 23, 2020, https://www.hpnonline.com/infection-prevention/article/21146786/what-we…
Tara Ragu, Rachel Werner, & Andrew Artenstein,, “Why don’t hospitals have enough masks? Because coronavirus broke the market.” Washington Post, May 21, 2020 https://www.washingtonpost.com/outlook/2020/05/21/why-dont-hospitals-ha…
BEA, “Gross Output by Industry,” BEA, accessed November 2020, https://www.bea.gov/data/industries/gross-output-by-industry
USITC, “Us Trade Balance Data,” USITC, accessed November 2020, https://dataweb.usitc.gov/
IBIS World, “Medical Supplies Wholesaling in the US,” IBIS World, October 8 2020, https://www.ibisworld.com/industry-statistics/market-size/medical-suppl….
Patrick Van den Bossche, Brooks Levering, Yuri Castaño, and Brandon Blaesser, “Trade war spurs sharp reversal in 2019 Reshoring Index,” Kearney Consulting Group, 2020, https://www.kearney.com/operations-performance-transformation/us-reshor…
Alberto Abadie, Alexis Diamond, and Jens Hainmueller, (2015), “Comparative Politics and the Synthetic
Control Method,” American Journal of Political Science 59(2), https://onlinelibrary.wiley.com/doi/abs/10.1111/ajps.12116
Burel, G., “The Early Years,” October 9, 2019,
Burel, G., “Evolving the Scope,” November 27, 2019,
Burel, G., “Looking Ahead,” December 25, 2019,
Sarah Fitzpatrick, “Why the Strategic National Stockpile isn't meant to solve a crisis like coronavirus,” NBC News, March 28, 2020, https://www.nbcnews.com/health/health-care/why-strategic-national-stock…
Clark, D.B., “Inside the Chaotic,” November 17, 2020
Hersh, J., “Classified Stockpile,” March 17, 2020,
Patel, A., D'Alessandro, M., Ireland, K., Burel, W.G., Wencil, E., and. Rasmussen, S., “Personal Protective Equipment,” June 2017
Carias C, Rainisch G, Shankar M, Adhikari BB, Swerdlow DL, Bower WA, Pillai SK, Meltzer MI, Koonin LM. “Potential demand for respirators,” May 2015
Slack, D., and Voyles, D., “US never spent enough on emergency stockpile, former managers say,” [Updated link on March 10, 2026] USA Today, March 27, 2020, https://www.usatoday.com/story/news/investigations/2020/03/27/u-s-never…
Hersh, J. “US Classified Stockpile,” March 17, 2020
Hersh, J. “US Classified Stockpile,” March 17, 2020
Greenfieldboyce, N., “Inside A Secret Government Warehouse,” June 27, 2016
Groll, E., “The Defense Production Act Won’t Fix America’s Mask Shortage,” Wired, April 6, 2020, https://www.wired.com/story/defense-production-act-n95-masks-shortage-c…
McSwane, J.D., “How Profit and Incompetence Delayed N95 Masks While People Died,” ProPublica, May 1, 2020, propublica.org/article/how-profit-and-incompetence-delayed-n95-masks-while-people-died-at-the-va
AP Pool Report, “Trump administration tries to narrow stockpile’s role for states,” LA Times, April 3, 2020, https://www.latimes.com/world-nation/story/2020-04-03/trump-admin-tries…
Clark, D.B., “Inside the Chaotic,” November 17, 2020
Clark, D.B., “Inside the Chaotic,” November 17, 2020
Finkenstad, D.J., Handfield, R., and Guinto, P., “Why the U.S. Still Has a Severe Shortage of Medical Supplies,” Harvard Business Review, September 17, 2020, https://hbr.org/2020/09/why-the-u-s-still-has-a-severe-shortage-of-medi…

About Justin Myers
Justin is a senior from Omaha, Nebraska majoring in economics with minors in national security and political science